
Kent: We had spent a fair amount of time in South Asia and had seen many surprising and sometimes startling sights; but this was still unexpected. As the light faded and the heat dissipated, the scene could almost have been set by Merchant and Ivory themselves: Sarah and I sipped tea and watched people finish their day’s viticulture. But this was no ordinary vineyard, and the men in the fields were bound together by more than just horticultural skills.
It is 2008 and we are two hours outside of Islamabad in rolling and verdant lands that produce fine table grapes. The lack of fermentation isn’t the only thing that distinguishes this vineyard from its Mediterranean peers. The men tending the vines are recovering drug users, and working in exchange for the security of being part of Nai Zindagi, Pakistan’s largest non-governmental organization (NGO) providing harm reduction services for injectors.
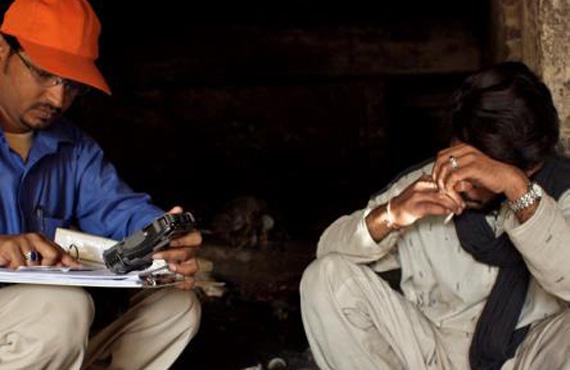
Sarah: For two years we have been working with Nai Zindagi to reach out and recruit the most marginalized citizens to participate in a study of HIV and other sexually transmitted infections. We were enrolling people who used drugs, sex workers (male, female, transgender people) and their clients. It was a large interdisciplinary study –a mix of Pakistani and British scientists spanning methods (behavioural science, molecular diagnostics, mathematical modelling, and more) and continents. Almost 2000 members of “most at risk populations” were recruited, thousands of clinical samples collected, tens of thousands of pieces of information analysed. A picture began to emerge of the evolution of sexually transmitted infection epidemics in the Islamic Republic.
The transgender people have the highest prevalence of syphilis that had been recorded, high levels of risk, and even higher levels of vulnerability. In-depth interviews analyzed by social scientists highlight that the trans-women find solace amongst themselves. They live in houses with other trans-women, often with a strong “mother figure”. This was important, they told us, because it gave them a sense of family and community. However, like the male sex workers, they have no political voice, and their position in society is precarious, often dependent on the whims of police officers: one in five tells us she has been raped by the police in the past year (with more providing “free sex” to the officers)
Our two-year study uses state-of-the-art technology—Pakistan has some incredible high-tech GPS-enabled data collection tools. We have real-time data, molecular diagnostics in a quality-controlled laboratory in Karachi, and amazing satellite maps convincing us of the theory of “hot-spots” as sites of risk-taking.
This allowed us to gather highly accurate data about the current and potential status of sexually transmitted infection epidemics in Pakistan. The data are clear: it is a relatively young epidemic, still concentrated among people with highly vulnerable behaviours, but the numbers tell a more sobering story. Without action, the HIV epidemic will spread, and the most vulnerable will be transgender sex workers, followed by male sex workers. Drug users are at risk, but their situation is modified (at least in the mathematical models) by their access to effective programmes – harm reduction services have been provided by Nai Zindagi since 2000, and their amazing efforts seem to be paying off, at least in the cities we surveyed.
The conclusions are presented to the Government and sponsors: harm reduction for people who inject drugs works and sex workers are highly vulnerable and they need immediate access to effective HIV prevention and treatment services. Also, training programmes for police officers could be a step to stop the human rights abuses that had been reported.
The National AIDS Control Programme nod their heads in agreement but are concerned about how to implement them. “This is Pakistan”, they say. They agree that the conclusions are based on sound evidence and that the results of the modelling show how far and how fast the HIV epidemic could spread, particularly among the male and transgender sex workers. The evidence is sound and the conclusions very sobering. “But this is Pakistan”, they remind us and providing services for people who live on the [illegal] margins is not likely to be at the top of the political agenda.
Kent: So Sarah asks me, “Is there some way we could make the recommendations a little more feasible?” I construct a simple framework with 15 variables which ought to give good sense of the political palatability of each of the recommendations. We then conduct a series of face-to-face interviews with decision-makers in the Pakistani health policy arena.
Respondents give voice to fears about the likely reception towards our recommendations: programmes for drug users and female sex workers will be well received, with little opposition likely. Proposing to channel resources to services for men or transgender people who have sex with men, however, lack support, and will almost certainly meet with opposition. In the words of one Senator, “Pakistanis will eat bacon before they publicly condone let alone decriminalize such behaviour”.
Sarah: Dr Hasan Abbas Zaheer, the head of the National AIDS Control Programme, suggests a middle way—a set of recommendations that won’t result in immediate services for vulnerable communities, but may foster a more sustainable impact in the longer term: community empowerment programmes. He says that rather than trying to impose services from the top, resources would be better spent building demand for service provision. It was an approach which I respected.
Kent: DFID, the sponsors, promise to consider both the evidence and the politics.
The following year the Global Fund awards $3 million to the Naz Foundation to support their work with men who have sex with men and transgender communities. They will provide services and foster communities who will slowly change social norms and demand modest change from below.
While the rehab vineyard may have been surprising, the policy process was not. Evidence doesn’t always speak for itself; nor does it always lead to a big bang of policy change. But any evidence-informed step forward is a step in the right direction.
Contributor

Sarah Hawkes is Reader in Global Health at the Institute for Global Health, UCL, and Wellcome Trust Senior Fellow in Public Engagement. Sarah is a specialist in gender and sexual health, with a focus on Asia and the Middle East, and lived for many years in India and Bangladesh. She works extensively with international organizations and with Ministries on evidence-informed policy development.
Kent Buse serves as Chief, Political Affairs and Strategy at UNAIDS. He is a political economist who has taught at Yale University and at the London School of Hygiene and Tropical Medicine. He is author/editor of a number of books including Making Health Policy, Making Sense of Global Health Governance and Thinking Politically about HIV.
What keeps them hopeful? “An abiding belief that injustice is solvable; collective action can make the world a better place for everyone.”
Post a comment